Femoral- Above the knee Popliteal Bypass Graft

Introduction
What is it?
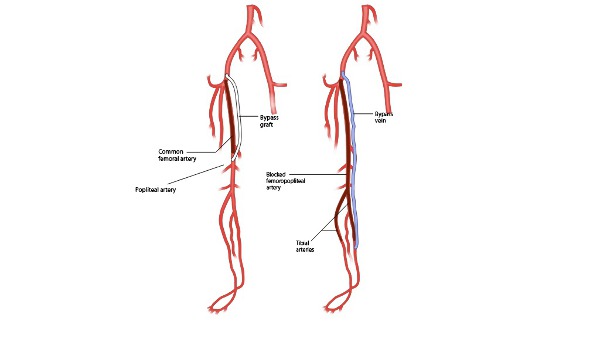
Leg surgical bypass involves stitching a vascular conduit (pipe routing blood flow), ideally patient’s own vein, from a site on the artery above the level of an arterial occlusion to a site on the non-diseased artery blow the blockage. A Femoral-above-knee-Popliteal bypass is performed by anastomosing (attaching) a conduit (pipe) between the Common Femoral artery in the groin and the Popliteal artery in the thigh (above the knee).
Why is it done?
The most common reason to do a leg surgical bypass graft operation is peripheral artery disease (PAD) due to a disease called atherosclerosis (narrowing of the arteries).
Patient can have a range of problems with PAD. Problems can range from pain on walking on the affected leg which disappears after stopping for a few minutes (called Intermittent Claudication), to ulceration or gangrene of the foot.
Intermittent Claudication.
Patients with Intermitted Claudication are initially treated with exercise therapy. Supervised Exercise Programme under the supervision of trained staff have been shown to significantly improve the amount you can walk after 3 to 6 months of training.
However, if these symptoms deteriorate to a point that they significantly affect daily life or even further to cause 'Rest Pain' in the foot or gangrene or ulceration then bypass can be considered.
Critical Limb Ischaemia (CLI).
Ulceration of the skin or 'Rest Pain' or gangrene which is persistent due to lack of blood supply is called 'Critical Limb Ischemia' (CLI).
Critical Limb Ischaemia (CLI) usually needs urgent revascularisation - ie reconstructing the blocked blood supply. either via endovascular (key hole technique) or bypass surgery to save the leg.
Aneurysm.
Other indications for Femoral- Above the knee Popliteal bypass include Femoral artery aneurysms (abnormal swelling of the Femoral artery). Traumatic injury to the arteries in the groin or thigh resulting in bleeding or blockage may require a bypass to be done.
BASIL trial comparing bypass to endovascular surgery.
The Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial is the only randomised study comparing open surgery with endovascular treatment, and showed no significant difference between endovascular or open surgical options for patients with critical limb ischemia with femoral artery occlusion in the first 2 years but the bypass graft performs better after two years in terms of its durability and amputation free survival [1]. Although the numbers in the trial were not conclusive to say, there was a suggestion that bypass following failed endovascular treatment had a worse outcome than where bypass was done initially.
Will I need to do any preparation?
Optimisation of risk factors.
Risk factors for PAD include advanced age, smoking, high cholesterol and diabetes. Fifteen percent of people older than 70 suffers from PAD [2]. These risk factors results in a higher risk of having problems with the heart, lungs and blood supply to the brain. Therefore a thorough assessment needs to be carried out to assess fitness for surgery.
This may involve their risks to be optimised by medicines including Aspirin or Clopidogrel and Statin therapy. Also by stopping smoking and exercise therapy.
Echocardiogram (heart scan) and lung function tests are sometimes done as part of pre-operative assessment for surgery.
Choices with regards to treatment options are discussed on the basis of assessment in clinic, the pre-operative assessment tests and further tests to assess the anatomy of the blood vessels.
The anatomy of the blood vessels is checked using a combination of Arterial and Venous Duplex ultrasound scanning, Computed Tomographic angiogram (CTA) and/ or Digital Subtraction percutaneous Angiography (DSA) of the leg arteries. These tests provide a roadmap to decide on actual strategy with. They identify the location of arterial blockage and identify the down-stream target artery for bypass anastomosis.
The scan of the veins helps decide if your own saphenous veins are available to use for bypass. Alternative conduits used are the artery from your arm (radial artery) or artificial materials like expanded polytetrafluoroethylene (ePTFE), polyester or Dacron (Goretex). These are generally used if a vein is either not available or not of appropriate diameter, length, and quality for bypass durability.
Technique
Anaesthesia
Procedure is usually performed either under general anaesthesia or regional anaesthesia (spinal anaesthesia).
What does it involve?
The length and extent of the arterial blockage and well as the fitness of your heart and lungs are important consideration with regards to the decision making for bypass or angioplasty procedures. The operation can be thought of as a number of steps: 1. Preparation of the inflow artery; 2. preparation of the outflow artery; 3. Tunnelling and attaching the graft; 4. Quality Control.
1. Preparation of Inflow artery
Lower limb bypass grafts are usually done using a pipe or conduit between a healthy artery above and a healthy artery below the blockage. The Common Femoral artery in the groin is usually the site used to attach the top of the bypass graft to (proximal anastomosis). The exact artery chosen is called 'the inflow vessel'.
It is important to check that the arteries above the Common Femoral Artery are healthy and not narrowed prior to performing the graft. Narrowing upstream will cause poor flow and may contribute to the graft clogging up and failing.
In some cases the Femoral artery in the thigh or even the Popliteal artery around the knee is used as the inflow vessel for the bypass. This shortens the length of the bypass which is better for longer term outcome.
2. Preparation of the outflow artery
The Recipient artery for the graft need to be disease free and is termed outflow vessel and is the site for distal anastomosis (join). Outflow vessel should ideally have a directly un-obstructed path all the way down to the foot in order for the foot to get adequate blood flow. Vein is harvested, prepared to be used as a conduit.
3. Tunnelling and attaching the graft.
If at all possible, a vein is 'harvested' from your own leg or arm to use as the conduit (pipe). Either multiple incisions or single long incision is made to 'harvest' the vein in your leg.
To route the bypass in the leg a tunnel needs to be created in between the muscle layers of your leg or in the fat between the skin and the muscles. Effort is made to make the path of the graft in the tunnel to be smooth and without kinks.
Proximal and distal anastomoses (top and bottom connections) are sewn using fine stitching with specialised instruments.
3. Quality Control.
Duplex ultrasound or completion angiogram or hand help Doppler assessment is performed after the completion of the bypass to confirm that it is working well.
How long does it take?
The operation can take up to 4 hours or more depending on complexity.
Post procedure course (follow-up)
Surgeon may consider patient to be on an aspirin / clopidogrel or an anticoagulation therapy time post operatively [3]. Statin therapy has also been associated with improved infrainguinal graft patency [4]. Postoperatively a duplex ultrasound scan of the graft is performed to assess patency prior to discharge from the hospital. This scan acts as a baseline reference for the future and also helps assessing any problems with the graft (narrowing or sluggish flow). During the follow up in the clinics some surgeon prefers surveillance of the graft using duplex ultrasound scan and others prefer to do ankle brachial pressure measurement and clinical examination only.
How long does it take?
Operation can take up to 3 hours or more.
Post procedure course (follow-up)
Surgeon may consider patient to be on an aspirin / clopidogrel or an anticoagulation therapy time post operatively [3]. Statin therapy has also been associated with improved infrainguinal graft patency [4]. Postoperatively a duplex ultrasound scan of the graft is performed to assess patency prior to discharge from the hospital. This scan acts as a baseline reference for the future and also helps assessing any problems with the graft (narrowing or sluggish flow). During the follow up in the clinics some surgeon prefers surveillance of the graft using duplex ultrasound scan and others prefer to do ankle brachial pressure measurement and clinical examination only.
How long will I stay in hospital?
Usual hospital stay is around 7 days.
When can I start my normal activities again (e.g. driving, sports or work?)
Returns to work normally between 6 to 12 weeks and patient should be able to drive after 4 to 6 weeks.


Comments