Laparoscopic Splenectomy
Description
Laparoscopic Splenectomy is a minimally invasive surgical procedure involving the removal of the spleen. It is used in the treatment of a wide range of haematological disorders, and is usually conducted after medical treatment has failed.
There is a significant preoperative protocol that needs to be followed; with particular emphasis on providing immunisations against specific respiratory infections. The surgery is carried out under general anaesthetic and recovery involves pain relief and a gradual easing back into day to day activities. Long term care is required due to the loss of immune function as a result of splenectomy, which most commonly includes the provision of a life-long course of prophylactic antibiotics alongside regular vaccinations.
Complications of the surgery can be severe and include intra-peritoneal haemorrhage alongside infection and sepsis. Severe infection in the form of Overwhelming Postsplenectomy Infection (OPSI) can also occur, which has a rapid onset and requires immediate medical attention.
What is it?
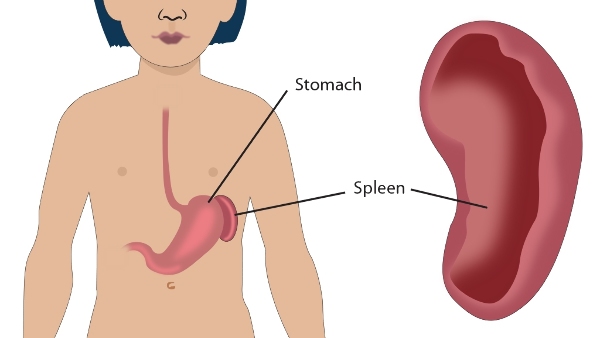
The spleen is an organ located in the upper left part of the abdomen, which performs a number of functions related to the blood including:
- Removing old red blood cells and recycling their contents.
- Hosting special immune cells called phagocytes which can engulf and destroy bacteria.
It may be necessary to remove the spleen due to a number of haematological (blood related) disorders and trauma related factors. Laparoscopic Splenectomy refers to the minimally invasive surgical procedure of removing the spleen.
Why is it done?
Laparoscopic Splenectomy is conducted for a number of different reasons that necessitate removal of the spleen. Often, medical and more conservative treatment is trialled first; yet if the disease fails to respond to this treatment, then removal of the spleen may be required to prevent further deterioration in your health. Reasons for removing the spleen include:
- Following bleeding or rupture of the spleen after traumatic injury (1).
- To help treat haematological diseases where the splenic function is disrupted resulting in a breakdown of red blood cells (haemolysis). There is a whole range of both inherited and acquired haematological disorders that involve splenic disease including:
- Auto-Immune Thrombocytopenic Purpura (ITP) - This is one of the most common reasons necessitating removal of the spleen and involves the body having an abnormal response to platelets in the blood. These platelets help with clotting when there is a bleed, and in ITP this function is disrupted and the platelets are destroyed in the spleen. Hence should medical therapy fail, then splenectomy may be required to restore the ability of the body to clot and stop bleeding (2).
- Haemolytic Anaemia - This involves a number of different conditions which result in the breakdown of red blood cells in the spleen. Hence removal of the spleen may be required to restore your red blood cell count (3).
- Hereditary conditions such as spherocytosis and thalassemia - These diseases typically result in abnormal red blood cells, which are then destroyed by the spleen, much like in Haemolytic Anaemia.
- To help treat haematological cancers such as Lymphomas and Leukaemias (4).
- When the spleen has enlarged in size (splenomegaly) to such an extent that it is interfering with daily activities through discomfort and pain. This can be either as a result of benign or more serious conditions (5).
- If cancer has occurred elsewhere in the body and has spread to the spleen (metastasis). This is more common in specific cancers such as ovarian cancers (6).
Anaesthesia
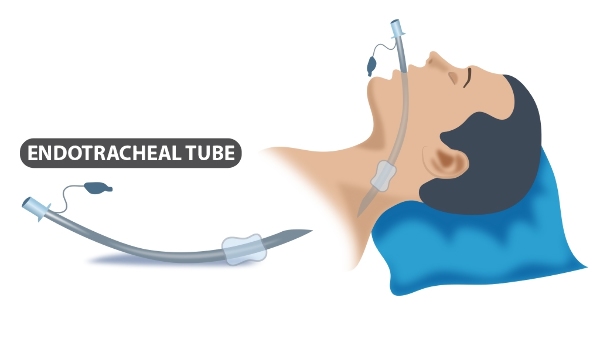
Before the procedure, you will have an appointment with an anaesthetist in a pre-admission clinic where you will be able to discuss the method of anaesthetic to be used in the surgery, alongside any options for pain relief after the operation. The surgery is usually conducted under general anaesthetic, which means you will be unconscious through the surgery. An endotracheal tube will therefore be required to be placed down your throat to help with breathing during the surgery as shown below.
Will I need to do any preparation?
There is a wide variety of tests that may need to be conducted before the operation to ensure that you are capable of dealing with reduced immunity after the procedure. Furthermore, tests will be conducted to ensure correct diagnosis before the splenectomy is conducted. These include:
- Blood tests - While standard full blood counts will be ordered, specialist tests such as kidney function tests may also be performed.
- Lung Function tests and ECG - These will be conducted to ensure you are fit enough to undergo major surgery.
- Bone Marrow Biopsy - This may be necessary to look at the development of blood cells and to assess whether a haematological tumour such as a leukaemia or lymphoma is present.
- Imaging of the spleen - This is done through either a CT or MRI scan and helps to visualise the spleen and diagnose the disease. Imaging is particularly useful in determining the size of the spleen which may influence the decision as to whether to use an open or laparoscopic approach. CT scans are also particularly useful if any accessory spleens are detected, which are areas of splenic tissue occurring outside the spleen in the abdominal cavity and which may require removal (11).
The spleen is heavily involved in the immune regulation of the body as it contains specific cells called macrophages which destroy invading bacteria. Hence the main issue post-splenectomy is a lifelong increased risk from infections; particularly respiratory and neurological infections e.g. pneumonia, meningitis etc (12).
To reduce the risk of any infections post-splenectomy, your doctor will talk to you about different steps that can be taken. One of the major steps is providing regular immunisations to protect against the most common and serious infections. Ideally, these will be given 2 weeks before the operation is scheduled to take place. Hence these vaccinations will be scheduled for you at your local GP after discussion with the haematological doctors and surgical team. If giving these vaccinations before the surgery is not possible, particularly in emergency situations, then the course of immunisation can be given as soon as possible post-operation. The different vaccinations include:
- Pneumococcal immunisation (to protect against streptococcus pneumoniae)
- Haemophilus influenzae type b immunisation
- A course of Meningitis vaccinations
- Annual Influenza vaccination (13).
If you are a smoker, you will be given advice on stopping smoking. This will greatly increase the likelihood of successful surgery and help to reduce the chance of any complications arising.
You will be required to not have anything to eat from the night before your operation, and you can only have small sips of water on the day of your operation.
The Surgery
The steps of the surgery are as follows:
- You will be placed under general anaesthetic and an endotracheal tube will be passed down your throat to help you breathe while you are unconscious. The surgeons will then position you to enable access to the spleen during the surgery. The choice of position depends on your individual case alongside surgeon preference. The majority of surgeons prefer either the hemilateral or lateral position where you are placed on your right hand side to allow for the best view of the spleen on the left hand side of the body.
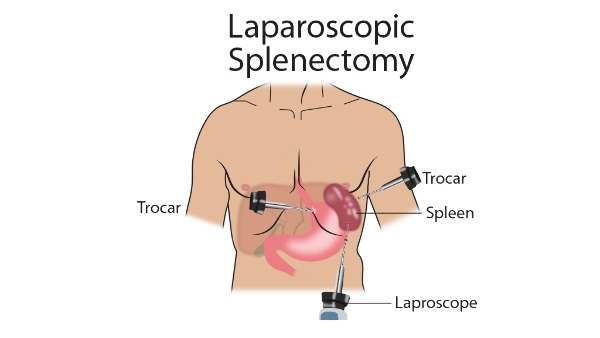
- Incisions are made in your abdomen to allow for the different pieces of equipment to enter. Usually three incisions are made in the upper left region of your abdomen as shown below.
- A hollow tube called a cannula will be inserted through one of these incisions, and gas will be pumped in. This causes the inside of your abdomen to inflate during the surgery, thus allowing more room for the surgeon to operate and giving them a better view of the spleen and any associated structures.
- A laparoscope is passed through one of the incisions. This is a thin tube that has a video camera on its tip which sends live video of the inside of the abdomen to a TV monitor for the surgeon to view.
- The surgeons will begin the operation by searching for any accessory spleens. These are areas of splenic tissue that occur outside the spleen, and may be found in up to 15% of people. They are typically found in the associated structures of the spleen and its blood vessels, or in other areas of the abdominal cavity. If any accessory spleen tissue is found, these will be resected and removed using a sharp cutting instrument such as a scalpel.
- Any adhesions or attachments connecting the spleen to the surrounding abdominal wall will be cut to allow the spleen to be mobilised and removed. This allows the surgeons to access the area of the spleen known as the hilum, which is a collection of blood vessels that enter and leave the spleen.
- The hilum of the spleen is cut using an endoscopic stapler, and bleeding is controlled with the use of surgical clips or medical agents.
- Once the hilum of the spleen has been completely divided, and any attachments resected, it can be removed and placed inside a recovery bag. This bag will be pulled through the largest incision made into your abdomen (14).
Post-operation
After the surgery has finished, you will be transferred to either a recovery ward or to the high dependency unit depending on the view of the anaesthetist while you recover. You will be given intravenous fluids in your arm, and your vital signs will be monitored and given pain relief. You can expect to spend between 2-7 days in hospital before being discharged back home.
The laparoscopic approach results in less pain than the open approach, however you may still be given injections or painkiller tablets for the first few days to help with pain relief. Breathing may be difficult or painful after having a major surgery such as splenectomy; and hence while you are in hospital, the nurses and physiotherapists will work with you to ensure your lungs recover and to prevent collapsing of the lung due to insufficient breathing (atelectasis) (15).
Caring for yourself at home
Although you would ideally have been given the course of vaccinations before the operation, the pneumococcal vaccination will be required to be repeated every 5 years to ensure the immunity is kept strong. Alongside this, you will also be required to take a life-long course of prophylactic antibiotics which will help reduce the effects of infections. Please speak with your local GP to coordinate these and to ensure that these steps in your care plan are not missed (16).
Your doctor will talk to you about seeking help urgently if you develop infections; as due to your reduced immune response you may require hospitalisation so that stronger antibiotics can be given. The doctor may also provide you with a bracelet or medical alert card in case of emergencies such that if you are ever admitted to hospital, the medical staff will be alerted to the fact that you no longer have a spleen and hence require extra infection control care.
Due to the fact that splenectomy is a major procedure, it can take up to 3 months for a complete recovery, depending on the patient and their background. You can expect to resume driving 5-7 days after your surgery, and you can begin to do daily activities as you see fit. You will have regular follow-up appointments to check on the progress of your recovery, during which time you can discuss any concerns of questions that you may have with the doctor.
Where can I find more information
NHS information on Splenectomy - https://www.nhs.uk/conditions/spleen-problems-and-spleen-removal/
Comments