Laparoscopic Adrenalectomy
Description
Laparoscopic Adrenalectomy is a minimally invasive surgical procedure involving removal of either one, or both of the adrenal glands. The surgery is predominantly as a result of tumour formation either within the adrenal cortex (Conn’s or Cushing’s Syndrome) or the adrenal medulla (Pheochromocytoma).
The surgery is performed under general anaesthesia and full recovery time is between 2-4 weeks, with the patient being kept in hospital 1-2 days after the procedure before discharge. Depending on individual patient situations, and whether a bilateral adrenalectomy was performed, the patient may be required to take continuous lifelong medication to replace and maintain healthy levels of adrenal hormones; an integral part of the long term care that post-adrenalectomy patients require.
Complications of the surgery range from wound infections to more severe complications including damage to nearby visceral organs and heavy intraperitoneal bleeding.
What is it?
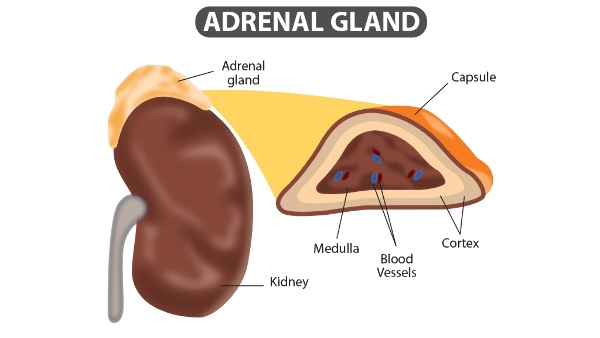
Laparoscopic Adrenalectomy refers to the surgical removal of the adrenal gland using minimally invasive “keyhole” surgery. The adrenals are a form of endocrine (hormone secreting) glands that are located above each of the kidneys. The adrenals are formed of many different layers broadly fitting into either the adrenal cortex (outer area) or adrenal medulla (core), with each layer producing a hormone that is vital to the continued functioning of the human body. These include:
- Aldosterone - This hormone regulates the level of salt in the body.
- Cortisol - This hormone is useful in the stress response.
- Adrenaline - This hormone is involved in your typical “fight or flight” response (1).
Either one or both of the adrenal glands are
removed in an adrenalectomy, depending on whether the disease has affected both
the left and right adrenals.
The removal of the adrenal glands can either be performed through a laparoscopic (minimally invasive) or open (invasive) approach. The exact procedure conducted depends on a combination of both patient factors and surgeon preference. One of the main factors which determines the choice of approach is the exact nature of the tumour. The tumours which are most suitable for removal via laparoscopic approaches are benign tumours such as adrenal adenomas and pheochromocytomas (2).
Why is it done?
Laparoscopic Adrenalectomy is typically done to remove both benign and malignant tumours in either or both of the adrenal glands. These tumours may form in various different layers of the adrenal gland and typically result in excess production of either:
- Cortisol (Cushing’s Syndrome) - This may result in unexplained obesity, high blood pressure, diabetes, and skin issues.
- Aldosterone (Conn’s Syndrome) - This may result in high blood pressure and imbalances in blood potassium levels. Often this high blood pressure does not respond to standard medical treatment, and hence further tests and imaging are required which eventually detect this tumour.
- Adrenaline/Noradrenaline (Pheochromocytoma) - Excess production of these hormones can result in severe headaches, rapid heart rates, and cardiac problems. Pheochromocytomas are mostly benign tumours which occur in the medulla (core) of the adrenal glands (3).
Anaesthesia
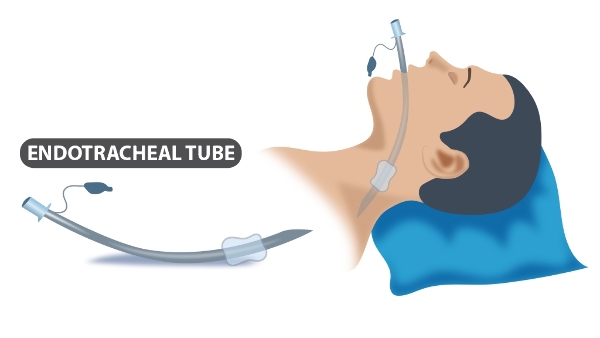
The procedure is formed under General Anaesthetic and typically lasts between 3-4 hours. On the day of your operation, you will meet the Anesthetist who will go through the procedure and discuss any concerns or questions you may have. Because general anaesthetic will be used, you will be unconscious throughout the surgery. As a result, an endotracheal tube will need to be placed down your throat to help you breathe (see diagram below).
Will I need to do any preparation?
Before your Laparoscopic Adrenalectomy, you will attend a pre-admission clinic with the surgeon to discuss the surgery and organise any tests that need to be conducted before the procedure is performed. You will undergo a series of steps to evaluate the tumour before the surgery. These are as follows:
- Biochemical testing of adrenal function - This is typically conducted via either a blood or urine test depending on the nature of the tumour suspected.
- Conducting scans to locate the position of the tumour - This may include X-Ray, CT, or MRI scans depending on the exact nature of the tumour (5).
- If your doctor suspects a pheochromocytoma, you may have to undergo a course of blood pressure medication involving alpha and beta blockers to make it safe for the surgery to proceed (6).
On the day of the surgery, you will be given some antibiotics to reduce the risk of infection during the procedure. In addition to this you will be given stockings to wear to prevent blood clots forming in the deep veins of your leg (Deep Vein Thrombosis). Patients undergoing an adrenalectomy may experience nausea post-surgery, and hence an antiemetic medication can be given to help with this. On the day of the operation you will be expected to fast from 6 hours before the operation, with not having anything to drink 2 hours before.
If you have been diagnosed with a pheochromocytoma and you have a family history of endocrine tumours, your surgeons may recommend genetic testing or scans of other parts of your body to check for the presence of inherited disorders such as Multiple Endocrine Neoplasia, although these are quite rare.
The Surgery
Laparoscopic Adrenalectomy can be performed in any of the following three methods:
- Transabdominally - This is where the surgeon enters through the front of the abdominal wall.
- Retroperitoneally - This is where a posterior approach (through your back) is used to access your adrenal glands.
- Transthoracically - This is rare and the surgery is only conducted in this manner when the tumours are very large such that they involve the diaphragm or have extended into the chest.
Transabdominal Adrenalectomy is often the approach of choice and can be conducted either in an open manner, or via laparoscopic minimally invasive techniques.
Laparoscopic surgery is a form of minimally invasive surgery that involves the use of a laparoscope (thin tube with a light and camera on the end). The camera sends live video to a TV screen in the Operating Room so the surgeon can see the area being operated on.
The steps of the surgery are as follows:
- On arrival for your surgery, the doctor will speak to you about the procedure and examine the area to be operated on. This is a good opportunity for you to ask any questions and raise any questions you have. You will then be given a gown to change into for the surgery.
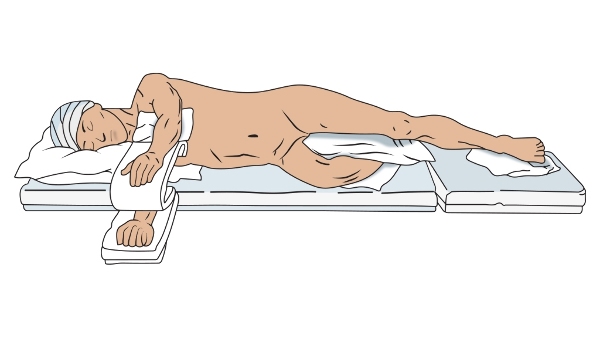
- At this point, the anaesthetist will go through some questions to determine if you are allergic to any medication, and will then administer the general anaesthetic. After being anaesthetised, you will be placed on a bed in the lateral decubitus position (see below). The exact side you will be placed on depends on whether the left or right adrenal is being removed at the time. You will be catheterised, which involves inserting a thin tube into your bladder, to allow accurate measurements of urine output.
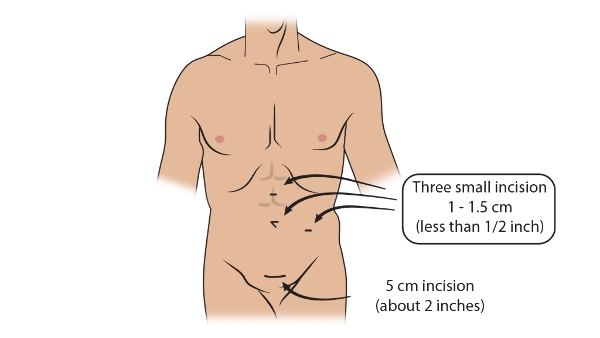
- At this point, the surgeon will mark the area where the incisions will be made. These incisions will be the sites in which the equipment necessary for the laparoscopic procedure such as the laparoscope can be inserted. Each of the incision sites will be sterilised using a special cleaning solution to minimise risks of infection. The sites of the incisions will differ depending on whether your left or right adrenal gland is being removed.
For a left laparoscopic adrenalectomy, three port incisions are made in the region of your abdomen under the left rib (subcostal region) to allow the pieces of equipment to enter (see below). For a right laparoscopic adrenalectomy, up to four incisions are made in the area of the abdomen under the right rib.
- Once the surgeons have gained access to the inside of your abdomen, they may pump some gas into the area. This will cause the abdomen to inflate and hence create more space for the surgeon to operate in and work with. The surgeon will first attempt to mobilise any surrounding structures, which involves dissecting any adhesions to give the surgeons a better view of the area. For a left adrenalectomy this includes mobilising the spleen, which will allow them to identify the left adrenal vein. For a right adrenalectomy, this includes mobilising a part of the liver known as the hepatic flexure. The surgeons will follow either the left or right adrenal vein to identify the relevant adrenal gland.
- For smaller masses, the adrenal vein is often dissected first and then the surgeon will move onto the actual adrenal gland. For larger masses, the surgeon may choose to dissect the adrenal gland first and then move down along the vena cava to reach the adrenal vein.
- The adrenal gland is dissected using a sharp instrument, while the small vessels including the adrenal vein are ligated using either electrocautery or using dissection. For a left adrenalectomy, dissection starts lateral (towards the outside of the body) to the spleen. For a right adrenalectomy, the dissection starts at the triangular ligaments which join with the liver.
- The adrenal veins and any other accessory vessels are ligated using surgical clips or sutures to prevent any postoperative adrenal bleeding.
- Once the adrenal gland has been fully dissected, it is removed through one of the port openings and placed in a bag for testing. One of the incisions may be widened to allow the adrenal gland to be fully removed without rupturing the skin or the organ (7).
If you have Cushing’s Syndrome and are undergoing an adrenalectomy; the surgeon may administer intravenous hydrocortisone once the adrenal gland is removed. This is to prevent adrenal insufficiency; whereby your body switches to producing insufficient adrenal hormones to maintain normal and healthy function.
Post-Operation
After the operation you will be taken to a recovery room to fully regain consciousness and be monitored. After a laparoscopic adrenalectomy without any complications, you can expect to stay in hospital between 1-2 days after surgery to recover. Post-Operative pain is common, particularly in the shoulder region and abdomen, hence you may be given patient-controlled analgesia while in hospital to help you regulate your own pain control.
Caring for yourself at home
Removal of the adrenal glands means that you may be required to continue taking adrenal hormones to compensate for the lack of adrenal function. This will particularly be the case if both adrenal glands are removed, or where only one is removed but there is limited capacity and functionality in the remaining adrenal gland. Hence before discharge, the surgeons will discuss and prescribe you with the appropriate medication to ensure you maintain a healthy level of hormones. It is important to continue taking these medications to prevent adrenal insufficiency (Addison’s Disease). These medications may include prednisolone to replace the cortisol, and fludrocortisone to replace the aldosterone (8).
Your doctor should explain to you about how to take these medications, particularly during periods of time where you may be more stressed than usual. During these times e.g. when you are going for surgery or experiencing personal stress etc, you should take more cortisol than your standard daily dose as you will lack regulation from your adrenal glands. This helps you compensate for the lack of adrenal function better (9).
You will be able to slowly return to your normal daily activities once your pain settles down, however expect full recovery to take between 2-4 weeks depending on the extent of surgery.
Where can I find more information
NHS information on Pheochromocytoma - https://www.nhs.uk/conditions/phaeochromocytoma/
Comments