Peripheral Vascular Disease in Diabetic Patients

Peripheral Vascular Disease in Diabetic Patients
What is peripheral vascular disease?
Peripheral vascular disease describes the narrowing and hardening of the arteries (which are vessels that take blood from the heart to the tissues) which branch from the aorta (the main central highway vessel leading from the heart). Peripheral vascular disease is ultimately defined by a reduction in blood flow through these arteries. This reduction in blood flow in the tissues is known as ischaemia. It represents a spectrum of disease which can progress to intermittent claudication (pain when walking) and ultimately long standing limb-threatening ischaemia.
The subsequent effect of a reduction in blood flow is determined by the organ or tissue that it occurs in. Most commonly, the reduction in blood flow to the muscles causes pain on exercising as there is insufficient oxygen delivery and removal of breakdown metabolites (which accumulate as the muscles use energy). The narrowing can progress sufficiently to cause pain at rest or breaks in the skin known as ulcers. If not treated, or if the disease progresses despite treatment, the end result can be gangrene of the tissues and limb loss. In those with diabetes, the vessels supplying the feet further down in the lower limb are more commonly affected (in comparison to non-diabetic patients). Furthermore, the hardening of the arteries can be more profound, this is commonly referred to as vessel calcification. The result of this is that peripheral vascular disease manifests in a different form in those with diabetes which means it requires a bespoke and multi-disciplinary approach when considering treatment.
What causes PVD?
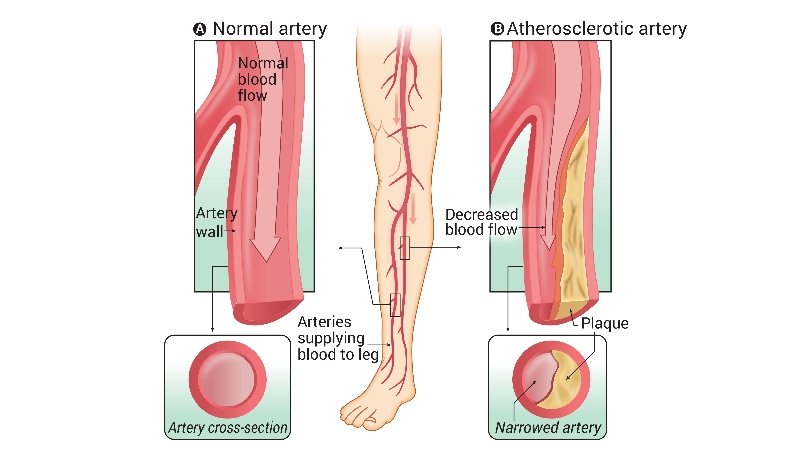
The cause of peripheral vascular disease is an interplay of genetic (susceptibility) factors with environmental (lifestyle) exposures. It represents a form of cardiovascular disease and is therefore more common in those that suffer from coronary artery disease (in the heart) and abdominal aortic aneurysms (which is disease of the large central vessels). The narrowing and hardening of the arteries is due to a process known as atherosclerosis. This is an inflammatory process in which certain cell types move into the artery wall and begin a chemical process which changes its structure. This process leads to infiltration of the artery wall with fat-like substances which are then chemically changed and harden over time. The artery wall is then vulnerable to plaque formation in which the inner surface of the artery is broken and fissured – this means it is more susceptible to narrowing and blockage. There is a wealth of research into this process and certain medications are targeted at halting and reversing it.
There are known risk factors which include cigarette smoking, poorly controlled high blood pressure, increased cholesterol, being male and increasing age. As with other complications of diabetes, poorly controlled blood sugar levels are likely to play a key role in progression of peripheral vascular disease.
How is PVD diagnosed
The diagnosis of PAD can be difficult, particularly in those with diabetes. Many will be asymptomatic, or trouble free, with “mild” peripheral vascular disease. Pain when walking, known as intermittent claudication, tends not to occur until at least 50% of the artery is narrow (known as a luminal stenosis of >50%). Furthermore, as blood vessels become increasingly narrow, other blood vessels increase in size, a process known as collateralisation. This compensates for the reduction in blood flow and can mean that those with marked severe peripheral vascular disease do not have dramatic symptoms.
Traditional investigations are primarily in the form of a clinical assessment in which a thorough consultation will establish if someone has any symptoms of peripheral vascular disease. Furthermore, examination to feel for the pulses in the legs will be undertaken and further assessment with hand-held doppler to determine the waveform of the blood flow are commonly undertaken.
From here, the following investigations are considered:
Ankle-brachial pressure indices (ABPI): this is a test that can be performed in a normal clinic room and involves compressing the arteries of the upper and lower limbs with a blood pressure cuff to assess the flow through them. In those with normal arteries in the lower limbs, the blood flow will be reduced at the same pressure as it is reduced in the upper limbs. However, it is known to be a poor indicator of peripheral vascular disease in those with diabetes and is generally not used. This is because diabetes causes calcification (or severe hardening) of the wall of the arteries in the lower limbs rendering the blood pressure cuff unable to compress the artery – this meaning that the test is unable to accurately compare it the upper limb arteries.
Ultrasound duplex scan: this is a non-invasive test that uses conventional ultrasound paired with blood flow assessment. This allows mapping of the blood-flow through the arteries of the lower limb and is very useful in those with diabetes. It generally takes around an hour to perform and is purely diagnostic rather than being used as a therapy.
CT angiogram: this is a computed tomography (CT) scan that uses contrast injected into a vein. The scan is timed to capture the arterial supply to the lower limbs. It is widely available and quick to perform and offers valuable anatomical information. However, it can be difficult to distinguish the flow of contrast to the dense calcification present in vessel walls and is therefore not as useful at imaging the arteries supplying the feet, particularly in diabetic patients. The scan uses ionising radiation so is not suitable for those that are pregnant. Furthermore, the contrast needed for the scan can cause some damage to the kidneys and may be avoided in those with kidney disease - which is more common in diabetic patients.
MR angiogram: his is a magnetic resonance (MR) scan that uses contrast injected into a vein. The scan is timed to capture the arterial supply to the lower limbs, in a similar way to the CT angiogram. It takes around an hour to perform and is not as widely available as CT angiogram.
Intra-arterial angiogram: this is when dye is injected directly into the artery and serial x-rays are taken in succession. The needle is placed through the skin under local anaesthetic. It uses ionising radiation and hence is not suitable for those in pregnancy. The dye provides excellent visualisation of the inside of the arteries and is very useful for imaging the arteries entering the foot. It also offers an opportunity to provide an intervention such as balloon angioplasty and stenting, however, it is invasive and is associated with complications (see percutaneous peripheral vascular interventions).
How common is PVD?
Peripheral vascular disease is common and affects an estimated 236.6 million worldwide. It is more common in those with diabetes in comparison to matched controls (meaning people who are similar in all respects apart from not having diabetes). It occurs in an estimated 9% of type 1 diabetics and as 24% of type 2 diabetes. There is significant geographical variation in the severity of peripheral vascular disease across the world and within, however, the evidence for this is not entirely clear. This is likely to be due to the organisation of services that specialise in the diagnosis, investigation and management of those with peripheral vascular disease and diabetes. For example, within the UK, there is evidence of significant geographical rates of lower limb amputation due to severe peripheral vascular disease and diabetes.




Comments