Laparoscopic Sleeve Gastrectomy
Description
Laparoscopic Sleeve Gastrectomy is a minimally invasive weight loss (bariatric) surgical procedure. It involves removal of the greater curvature and fundus of the stomach and hence is a restrictive weight loss procedure. It is one of the most commonly performed bariatric procedures and is associated with fewer complications than a typical Roux-en-Y gastric bypass.
The surgery is performed under general anaesthetic and recovery usually takes up to 4 weeks, during which time the patient is placed on a liquid diet to aid recovery.
Complications of the surgery range from postoperative leakage and bleeding which can occur even after 12 weeks, alongside more serious complications such as portal vein thrombosis. New onset gastroesophageal reflux disease is also a common complaint after the procedure and can usually be managed medically.
What is it?
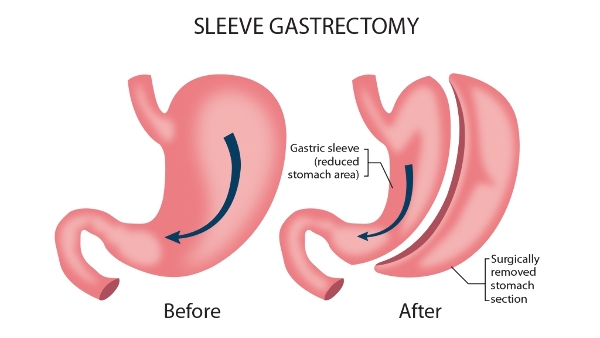
Sleeve Gastrectomy is a surgical procedure involving the removal of the greater curvature and fundus of the stomach (approximately 80% of the stomach). This results in the stomach holding a capacity between 90 - 220ml in comparison to the original 600 - 2000ml. It is a form of weight loss surgery (bariatric surgery) and is classed as a restrictive surgical procedure as it limits the amount of food that a person can eat before they feel full (1). The surgical procedure involves a vertical cut, resulting in the formation of a narrow tube that is less easily expandable than the original stomach. This narrow tube is what gives the surgery the name “sleeve gastrectomy”.
Why is it done?
Sleeve gastrectomy is one of the first line surgical procedures for patients wanting to lose weight. Patients will typically be obese with a BMI of >= 40kg/m^2, but can also be utilised in patients with a BMI of between 35 and 40kg/m^2 provided that there is evidence of serious co-morbidities resulting from the obesity (2). Laparoscopic Sleeve Gastrectomy helps the patient lose weight through two main methods:
- Restrictive approach - Due to the fact that after the operation the stomach has been vastly reduced in size and ability to expand, you physically will not be able to eat as much as you would have done before the procedure.
- Hormonal mechanism - There are a number of hormones secreted within the gastro-intestinal tract that contribute to weight control and eating. These hormones and their secretion are greatly effected on removal of large portions of the stomach and include:
- Ghrelin - This hormone is secreted in the fundus of the stomach and stimulates appetite, and hence removal of the fundus during a sleeve gastrectomy reduces ghrelin secretion and lowers appetite, making you eat less.
- Glucagon-like peptide-1 (GLP-1) - This hormone stimulates insulin secretion which increases satiety (causes you to feel full). Studies have shown how GLP-1 secretion is increased after a laparoscopic sleeve gastrectomy, causing you to feel more full and eat less than before (3).
Benefits of Procedure
Laparoscopic Sleeve Gastrectomy has been shown to provide high success rates regarding weight loss and other related conditions, alongside resulting in fewer complications than other bariatric surgical procedures such as a Roux-en-Y gastric bypass (4). Studies have shown that after 5 years post operation, patients lose 60.5% of excess weight alongside achieving an average BMI of 30.2 kg/m^2 (5). While the weight loss statistics may be slightly lower than for a Roux-en-Y gastric bypass surgery, the fewer complications often make a sleeve gastrectomy the surgery of choice for many patients. Furthermore, laparoscopic sleeve gastrectomy has been shown to result in much higher degrees of weight loss than non-surgical approaches, meaning that it can be used in patients where lifestyle changes and medical treatment has failed to result in adequate weight loss (6).
The surgery is done laparoscopically compared to being an open procedure, resulting in lower complication rates and quicker recovery times (7).
Anaesthesia
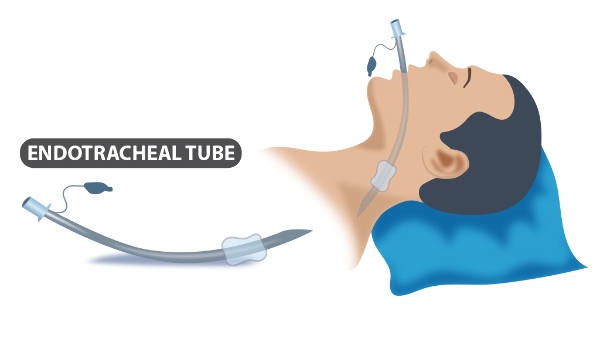
The surgery is carried out under general anaesthetic, which means that you will be unconscious throughout the surgery. For this reason, you will need to have an endotracheal tube placed down your throat to help you breathe during the procedure (see diagram below). You will have an appointment with the anaesthetist before the surgery where you can discuss any concerns or queries you may have, and go through any on the day procedures.
Will I need to do any preparation?
The preparation for bariatric surgery is often comprehensive, and involves both a psychological and physical component. This is performed in conjunction with nutritional assessments, and hence the preparation for bariatric surgery often involves multiple members of the multidisciplinary team.
An important aspect of bariatric surgery is ensuring that you are able and willing to make the lifestyle changes for the weight loss to be sustainable. Hence the psychologist will take into account factors such as previous attempts at weight loss, substance abuse, risky eating habits, and physical activity levels to assess whether you have the motivation required to make the necessary changes before and after surgery. The doctor will give you the appropriate advice to help you in this process, and may refer you to specialist nutritional and psychological services which will offer more specific help.
Before the procedure, you will need to undergo a comprehensive check-up and medical evaluation to exclude any other diseases that may make the surgery unsafe to proceed. While exact tests may vary on the patient, examples include:
- Barium Esophagram - This procedure involves swallowing a special contrast solution while having a scan conducted at the same time. This allows the surgeon to visualise any problems with the swallowing mechanism, alongside checking for any hiatus hernia (8).
- Esophagogastroduodenoscopy (OGD) - This is an endoscopic procedure regularly conducted in patients who are being considered for bariatric surgery. It involves inserting a thin tube with a camera into your mouth and then down your oesophagus. This allows the surgeon to assess for any other diseases within the oesophagus such as oesophagitis, as well as to test the patency of the gastroesophageal junction flap allowing entry of food contents into the stomach.
- Esophageal Manometry - This is used to test the motility and peristalsis functions of the oesophagus, alongside testing the function of the lower esophageal sphincter. This procedure is useful in patients who require further investigations to exclude other issues in the upper gastro-intestinal tract such as achalasia. While the presence of these diseases may not exclude a person from undergoing a laparoscopic sleeve gastrectomy, it is useful to know if they are present so that the surgeon can address them at the same time during surgery (9).
Before your operation, you will have a meeting with the surgeon who will go through the procedure and anything you need to do before the surgery day. You will be required to inform the doctor of any medications that you are taking, particularly any blood thinning medication such as warfarin and clopidogrel, as these may need to be temporarily stopped to reduce the risk of bleeding during the procedure. If you have diabetes, you will need to inform the doctor as your dose of insulin may need to be adjusted after surgery. Furthermore, if you smoke, you will be asked to stop ideally 12 weeks before the surgery is expected to take place to ensure the highest chances of success.
The Surgery
You will be given a gown to wear and brought into the operating theatre. The surgery takes between 1-2 hours, and starts once you have been anaesthetised. The steps of the surgery are as follows:
- Once you have been anaesthetised, you will be placed in the appropriate position. This is usually the supine position (lying on your back). The pressure parts and bony prominences will be padded to reduce the chances of any ulcer formation. To prevent any blood clots forming in your leg (Deep Vein Thrombosis), you may either have compression stockings placed on your legs, or a mechanical device that fits over your legs which may periodically compress your legs.
- At this stage of the surgery, the surgeon will clean the abdomen using a special sterilising solution, and will then begin making the incisions for the insertion of surgical equipment. While exact incisions may vary, common sites for incisions include:
- Subxiphoid area (usually in upper abdomen)
- Left Upper Quadrant
- Right Upper Quadrant
- Epigastric region (above your belly button)
- Once the incisions have been, gas may be pumped into your abdomen. This is done to allow your abdomen to expand and give the surgeon more room to work in and visualise the structures.
- The first stage of the surgery is to identify the pylorus of the stomach, which is the end portion of the stomach. This is done by identifying the prepyloric vein of Mayo. This step is crucial to ensuring that the beginning of the transection (dissection) is made further away enough from the pylorus such that the pyloric antrum is preserved. This ensures that any gastric emptying of food from the stomach into the small intestine takes place correctly.
- The next stage of the surgery involves mobilisation of the greater curvature of the stomach. This process involves devascularising this area to ensure no postoperative bleeding occurs by dividing the short gastric vessels and any other connecting vasculature. This step is important to ensure that the majority of the fundus of the stomach is transected away, resulting in the highest chances of success after surgery.
- At this stage of the surgery, the surgeon will assess for any hiatus hernia that is present. If the laparoscope (thin tube with a camera on the end) shows a hiatus hernia, this can also be repaired laparoscopically. It is important that the surgeon ensures that the left gastric artery is not divided, as this will be the only blood supply to the remaining portion of the stomach after the greater curvature and fundus have been removed.
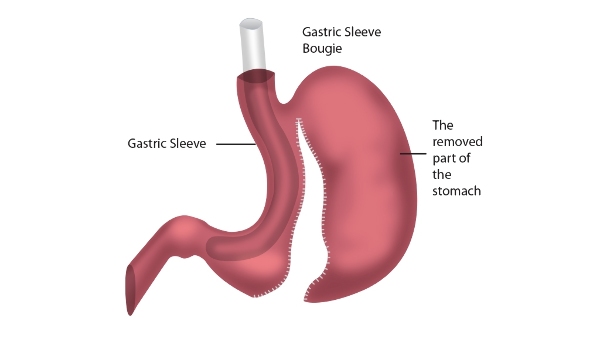
- A bougie (cylindrical piece of equipment) can then be inserted into the stomach and aligned with the lesser curvature of the stomach in order to guide the transection process.
- The transection of the stomach begins by applying a series of staples from a point 2-6cm from the pylorus upwards in a vertical fashion until the fundus is reached (10). The surgeon will take care not to twist the staple line which may narrow the sleeve and result in postoperative leakage. Furthermore, it is important that the surgeon does not place the last staple too close to the gastroesophageal junction, which can result in ischaemia of the area.
- The line of staples is sewn over to reduce the risk of any leakage, and the resected portion of the stomach is removed through one of the incisions. The surgeon can then perform an intraoperative leak test to ensure that the wound has been properly closed off (11).
Post-Operation
After the operation, you will be taken to a recovery room where you will be woken up and closely monitored. It is common to feel postoperative nausea after a laparoscopic sleeve gastrectomy, and hence you will be given intravenous antiemetics such as ondansetron to help with this (12).
You will be required to be admitted to hospital for overnight monitoring, and you can begin a clear liquid diet the morning after the surgery has been completed. A full liquid diet can then be started once you feel comfortable on a clear liquid diet, which will then have to be continued for two weeks while you recover at home.
Your doctor may want to perform a postoperative leak test which involves you swallowing a special contrast liquid while a scan is conducted of your stomach. However, your surgeon may not always perform this as most leaks occur well after discharge (13).
Caring for yourself at home
You will typically be off work for four weeks while you recover, during which time you may need to have someone else at home to help with any strenuous tasks. For the first two weeks you will need to remain on a full liquid diet. Before being discharged, teh dietician will help you with this and provide you with some food advice for sticking to this full liquid diet. After two weeks you can begin to eat pureed foods, and you can expect to eat normal foods after four weeks.
The removal of a large portion of the stomach means that you will be required to take nutritional supplements to compensate. These include iron and calcium supplementation, which will be prescribed to you on discharge. Your doctor will likely request you to have regular blood tests to ensure that your vitamin levels are kept within the healthy range. You may also be given regular lifelong Vitamin B12 injections which take place every 6 months.
You may feel some pain in your abdomen after the surgery. It is normal to feel some pain for the first couple of weeks as your body heals; this can be managed with painkillers. However, if you experience sudden or severe pain please seek urgent medical attention as this could indicate bleeding or a leak.
Where can I find more information?
NHS Information on Weight Loss Surgery - https://www.nhs.uk/conditions/weight-loss-surgery/types/
Comments