Carotid endarterectomy for asymptomatic patients

Why is it done?
The procedure is done to remove an area of narrowing in the Internal Carotid artery which supplied the brain. This area of narrowing is called an atheromatous plaque. The purposed of the procedure is to prevent small pieces of this plaque/ narrowing from breaking off and travelling up to lodge in the brain (embolisation). This embolisation can cause stroke or TIA (mini-stroke)
The Intended benefit is to reduce the stroke.
The benefit is the reduction in risk of ipsilateral stroke. The Asymptomatic Carotid Surgery Trial (ACST) and Asymptomatic Carotid Atherosclerosis Study (ACAS) reported a net reduction in stroke risk of 5.4% and 5.9% respectively over medical therapy over 5 years (1, 2). The ACAS and especially the ACST trials showed that the net benefit of carotid endarterectomy (CEA) is delayed, as the asymptomatic population has an overall worse outcome after CEA for many months up to 2 years because of the perioperative morbidity (2). The estimated risk of ipsilateral stroke in asymptomatic carotid atherosclerosis with stenosis more than 50% is approximately 0.5 to 1% annually (3). Multispecialty guidelines states that carotid endarterectomy should be considered for asymptomatic patients who have more than 70% stenosis of internal carotid artery if the risk of perioperative stroke, myocardial infarction and death is low (less than 3%) (4, 5).
Will I need to do any preparation?
Generally you will need to fast (not eat or drink) before the procedure. This is usually six hours for food and two hours for clear liquids. Taking blood thinning medicine is important to reduce the risk of clot building up on the rough area to be removed from the carotid artery.
Anaesthesia
The procedure can be done under general or local anaesthetic. Some surgeons prefer local anaesthesia because it allows direct monitoring of your brain function. If you are awake, you can be asked to talk to us or squeeze a ball in order to tell that your brain is receiving adequate blood supply (perfusion). Although a study has been performed which shows no significant difference in outcome from surgery performed under local or general anaesthetic, some surgeons prefer to perform the procedure under local for the ability to minimise the use of carotid shunting (see later).
What does it involve?
The procure involves a number of steps, not all necessarily need to be done depending on your individual situation.
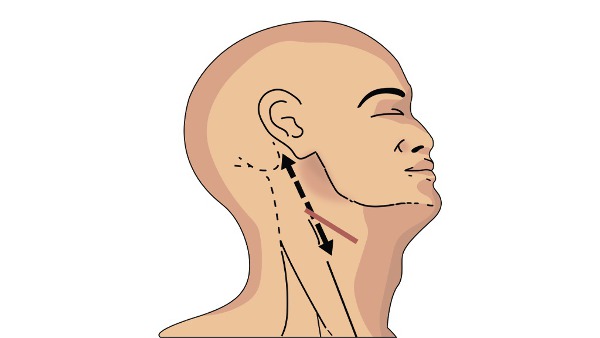
Firstly, you need to be comfortably positioned on the operating table. You will asked to look over to the opposite side to that being operated on to allow access to the neck.
The skin incision (cut) can be more vertical or more horizontal depending on the preferences of the surgeon. A more vertical cut allow better access to the structures being operated on whereas a more horizontal one tends to heal with a better scar.
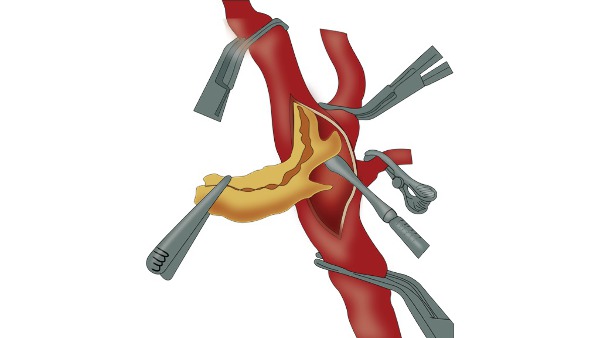
The next step involves freeing the Carotid arteries from the surrounding tissue. The main artery passing through the neck is called the Common Carotid Artery. This splits into two arteries (Internal and External Carotid arteries). The Internal Carotid artery supplies the brain and the External carotid artery supplied the side of the head, All three need to be freed up.
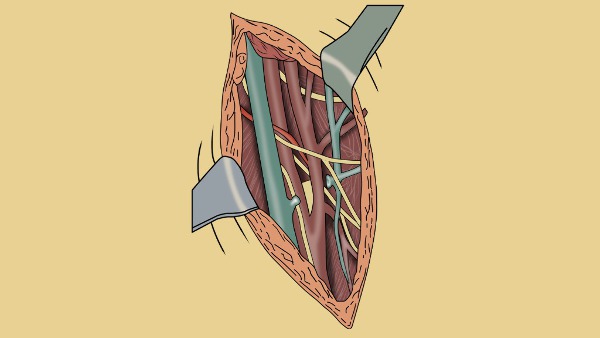
Care must be taken to free up the structures without damaging important nerves. The Vagus nerve lies between the artery and the vein. Damage to the Vagus nerve can cause a horse voice - this is usually temporary. The hypoglossal nerve above travels horizontally over the Internal and External carotid arteries. Damage to this cause weakness to one side of the tongue. This will cause the tongue to deviate to the damaged side when sticking it out. This is usually temporary also.
Once the arteries are freed up, heparin medicine is given to prevent blood clots building up in the blood when the arteries are clamped off. The arteries are clamped off and the diseased segment is opened. The narrowed area is cleaned - a process called endarterectomy.
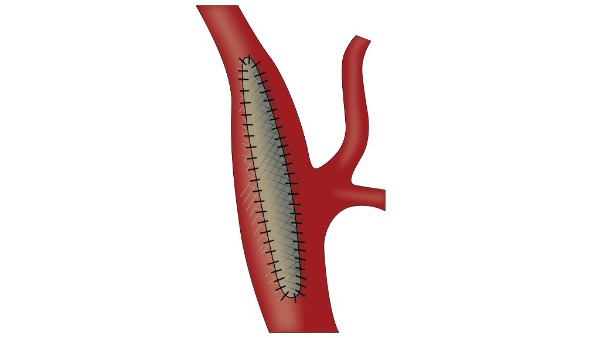
Once all the atheroma is removed and the inside of the artery is adequately cleaned, the artery is closed. This can be done directly with stitches or with a patch repair. It is important not to narrow the Internal Carotid artery when closing it - the patch can help with this.
How long does it take?
The procedure can take up to two hours normally. There will be additional time take for anaesthetic preparation and usually time spent after the operation in the recovery area.
Post procedure course (follow-up)
A drain may be attached to the neck to remove any fluid or blood that build up around the operation site for the first 24 hours. You may well be treated in the High Dependancy unit for the first 12-24 hours after surgery. This is done so your blood pressure can be accurately monitored using a monitoring device inserted into the radial artery at your wrist. If the BP strays high or low then this can be accurately treated which is important for the first 12 hours after surgery.
How long will I stay in hospital?
People often go home the next day following surgery.
What care will I need at home?
No particular care requirements are needed. The wound should generally be kept dry for around five days following the procedure and covered with a dressing. Whichever tablets your doctors have prescribed should be taken.
Will I need someone to stay with me?
No particular need, you should. be fully independant.
Will I need any special equipment when I go home?
No particular requirements.
What follow up care is needed?
Often a follow up Duplex ultrasound scan is performed to ensure no technical issues exist in the blood flow through the carotid artery.
When can I start my normal activities again (e.g. driving, sports or work?)
Normal activities can be started immediately. Driving should be discussed with your stroke physician as there may be specific restrictions on your activity following a stroke or mini-stroke.