Achilles Tendon Repair

Introduction
What is Achilles Tendon Repair?
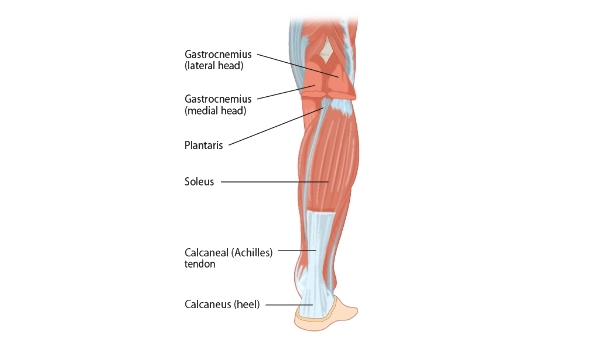
The Achilles tendon is the largest tendon in the body which connects the soleus and gastrocnemius muscles to the calcaneus (heel) bone. When these muscles contract, the foot points downwards and pushes off the ground, therefore a functioning Achilles tendon is important for running, jumping and accelerating/decelerating as well as walking and jogging.
The Achilles tendon ruptures (tears) under excessive stress,
commonly either during sports or athletics activity. The condition is
characterised by sudden pain, accompanied by a popping or snapping sensation at
the moment of injury. Thereafter, swelling may appear on the back of the leg,
and people often experience difficulty with walking. Tendon degeneration may
also result from poor blood supply, nerve disorders and autoimmune disorders.
Over 80% of Achilles Tendon Repair (ATR) cases are due to recreational sports,
and approximately 10% of cases have pre-existing problems with their Achilles
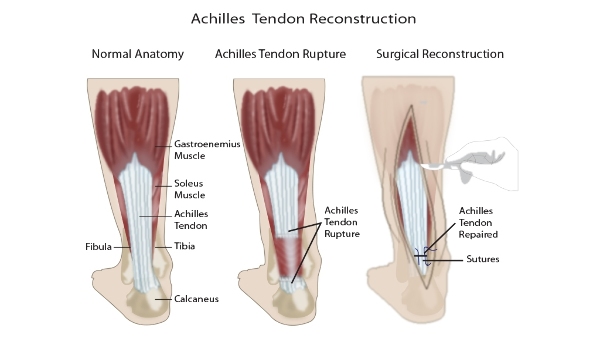
tendons (1). The tear may either be complete or partial, and each requires a
different management plan.
Achilles tendon repair involves making a small 6 cm incision on the inner side of the damaged tendon. The torn ends of the tendon are then strongly stitched together to ensure the correct tension is created. This procedure reduces the chance or re-rupture when compared to conservative (non-surgical) management (2).
Why is it performed?
Achilles Tendon Repair is indicated when the tendon has ruptured and cannot be repaired under conservative management. Repairing the tendon surgically can bring back a good level of function to the affected leg, which in athletes and sports people is a potentially life changing outcome. When the patient presents with a complete tear of the Achilles Tendon, ATR is always required. ATR can also be indicated for some patients with tendinopathy, which is defined as pain, swelling and impaired tendon function which is typically worsened on movement.
Achilles Tendon Repair Procedure
Anaesthesia
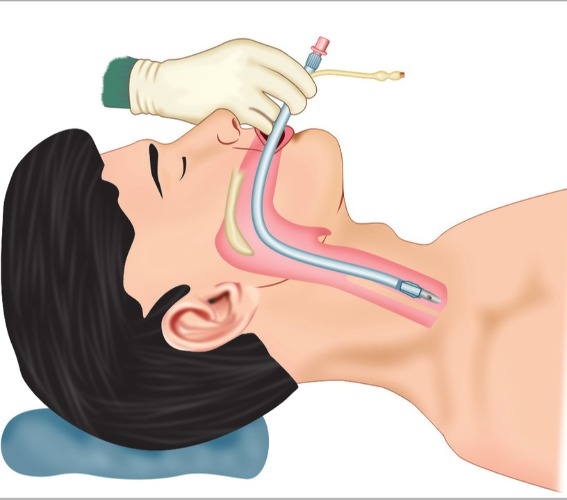
ATR is typically performed under general anaesthesia, which will mean that you will be asleep during the surgery and will not experience any pain. Your airway will be kept secure using an endotracheal tube, as demonstrated in the image below. This will ensure that you will not choke or breathe in any secretions which can lead to a chest infection.
Local anaesthetic is also injected into the ankle region to numb sensation during and after the operation, thereby relieving some pain postoperatively.
Pain control
The initial pain management of an Achilles Tendon Rupture involves applying an ice pack to the injured site, taking pain relief medication such as ibuprofen or acetaminophen and resting the affected leg. It is important to not put any weight on the damaged tendon, and your doctor will advise you with regards to how to use your crutches.
Will I need to do any preparation?
Prior to your surgery, you will be booked in to see a nurse who will assess whether you can safely undergo the surgery. You will be reviewed for the medications that you are taking, particularly herbal medicines, blood thinning medication and over the counter medications. Your full medical history will also be taken to assess for any previous injury to your Achilles tendon, or any other conditions which may be of significance.
Planning for recovery is another essential factor which will be discussed during pre-admission assessment. You will need to make the necessary preparations in the home and for living with a cast postoperatively. These include things such as ensuring you can get up and down stairs if you have them in your house, bringing things down from the shelves to make them easily reachable and arranging transport to and from hospital, as well as to shops and other places.
If the medical pre-admissions team have concerns over you being able to cope at home postoperatively, you may be referred to a physiotherapist or an occupational therapist to assess your needs and help make the necessary preparations. You will usually need to stay in the hospital overnight following the operation, so it is important to make transport preparations well in advance.
Steps of the surgery
An important factor which is considered for surgery is the timing of the operation. Surgery is usually performed within 1-2 weeks of the injury. Your surgeon will remind you of the surgical process and complication risks before asking you to sign a consent form. You will also speak with the anaesthetist who will be able to answer any queries you have about being given general and local anaesthetic. The surgery usually lasts between 45-60 minutes, and if no complications occur you will be able to return home the same day. Once again, the procedure will be performed under general anaesthetic, so you will be asleep before the actual operation begins. The method of repair outlined here is endoscopy-assisted percutaneous repair, which is a minimally invasive procedure.
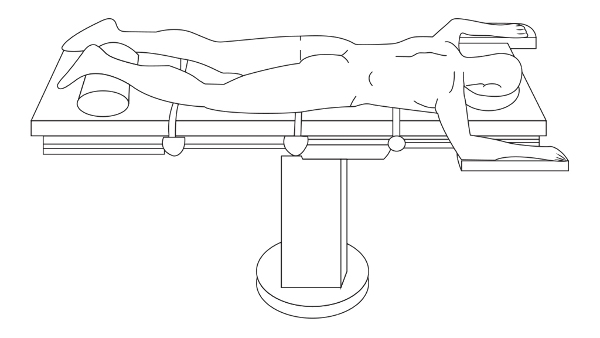
- You will be placed in the prone position, as shown in the image below. The rupture site will be marked.
- In order to minimize bleeding and numb region, a local anaesthetic will be injected above and below the injury site.
- 8 incisions are then made, four on the inner side and four on the outer side of the damaged Achilles Tendon. The incisions are then spread open wider using the ‘nick and spread’ technique which may reduce the risk of nerve damage during suturing.
- The damaged leg is then pointed upwards at approximately a 15-degree angle to give better access to the injured site.
- An arthroscope is then inserted via the incision closest to the inner border of the tendon. The images of the rupture and surrounding structures are then assessed for the level of damage and functioning blood supply to the tendon.
- Once the torn tendon has been inspected, a suture is passed through the Achilles tendon under the manipulation of the arthroscope. The tendon may be felt by the gloved hand of the surgeon to assess how effective the suturing of the tendon is. The AT can also be inspected throughout the suturing process to check for correct placement and potential bleeds.
- Finally, the sutures are tightened through the inner incisions and the suture is knotted.
- You will have a Vacoped boot fitted, which positions your foot pointing downwards. Once you have woken up and regained full consciousness, the staff will show you how to use your crutches, with special emphasis on the fact that you should not put weight on the leg in the cast.
Post-operative care and follow up
The suture method for repairing the Achilles Tendon is strong, thus rapid rehabilitation may be started.
You may begin walking with the crutches, placing the majority of your weight onto the healthy leg, so as to slowly ease your operated leg into mobilisation. Take pain relief as needed according to the advice of your doctor. Paracetamol and Diclofenac (NSAID) are suitable for mild to moderate pain, however when these two fail, you may be prescribed codeine, an opioid, which has a stronger pain relief effect. It is essential to keep the operated leg’s cast dry and keep it raised above the waist for the majority of the day.
At 2 weeks, physiotherapy through the outpatients department will begin. Your surgeon will see you in the outpatients clinic, and your wound will be inspected and stitches removed. Your leg will be fitted with an Aircast to facilitate you to begin bearing weight on the operated leg. From 2-8 weeks, the boot can be removed for bathing, physiotherapy and while seated. For all other times, including sleeping, the boot should remain on.
At 8 weeks you will be seen by your surgeon in outpatients again, this time to assess your Achilles Tendon healing, power, gait and ankle movement. You may be able to discard the boot and begin full weight bearing in your shoes. It may require 6 months or more to be able to return to sporting activities, and this should only be done with the full support and agreement of your surgeon. Rerupture is common in individuals that return to sports to0 early on in their recovery.
It is important that if you drive you have the ability to control the vehicle in emergency circumstances. This may range between 2-9 weeks post operatively, depending on your recovery rate. As always, your surgeon should be consulted prior to making this decision.
It’s imperative that you contact your GP or NHS 111 if you experience any of the following:
- Sudden cramping pain in the thigh, calf or groin
- Sudden pins and needles, numbness or increased swelling of the leg
- Any fluid seeping from the wound
- Fever
- Pain in the chest or shortness of breath
Where can I find more information?
https://www.nhs.uk/conditions/tendonitis/
https://www.londonfootandanklecentre.co.uk/condition/achilles-tendon-rupture/
https://patient.info/doctor/achilles-tendinopathy-and-rupture
References
- Leppilahti J, Orava S. Total Achilles Tendon Rupture. Sports Medicine. 1998;25(2):79-100.
- [Internet]. Ruh.nhs.uk. 2020 [cited 7 October 2020]. Available from: https://www.ruh.nhs.uk/patients/services/clinics/orthopaedic_fracture/documents/Acute_Achilles_Tendon_Rupture.pdf
- [Internet]. Ruh.nhs.uk. 2020 [cited 7 October 2020]. Available from: https://www.ruh.nhs.uk/patients/services/clinics/orthopaedic_fracture/documents/Acute_Achilles_Tendon_Rupture.pdf
- Jildeh T, Okoroha K, Marshall N, Abdul-Hak A, Zeni F, Moutzouros V. Infection and Rerupture After Surgical Repair of Achilles Tendons. Orthopaedic Journal of Sports Medicine. 2018;6(5):232596711877430.
- Keating J, Will E. Operative versus non-operative treatment of acute rupture of tendo Achillis. The Journal of Bone and Joint Surgery British volume. 2011;93-B(8):1071-1078.
- Pascoal D, Santos Silva M, Rosa J, Marques M, Correia B, Gomes A. Operative versus nonoperative treatment of acute Achilles tendon ruptures: Long-term study. Foot and Ankle Surgery. 2017;23:142.
- Wilkins R, Bisson L. Operative Versus Nonoperative Management of Acute Achilles Tendon Ruptures. The American Journal of Sports Medicine. 2012;40(9):2154-2160.
- Holm C, Kjaer M, Eliasson P. Achilles tendon rupture - treatment and complications: A systematic review. Scandinavian Journal of Medicine & Science in Sports. 2014;25(1):e1-e10.
- Bowers M, Turner N, Ryssman D. Outcomes following treatment of the infected Achilles tendon. Foot & Ankle Orthopaedics. 2018;3(3):2473011418S0016.
Comments