Laparoscopic Heller Myotomy (Cardiomyotomy)

Laparoscopic Heller Myotomy (Cardiomyotomy)
Laparoscopic Heller Myotomy is a surgical procedure used to treat achalasia, where the lower esophageal sphincter fails to relax and esophageal peristalsis is disrupted. During the procedure, the muscles of the lower esophageal sphincter are cut, allowing food to pass into the stomach. The procedure is often performed in conjunction with a Nissen Fundoplication to prevent postoperative reflux. It is the only treatment for achalasia that provides long-term relief and hence is often the treatment of choice for patients who can tolerate surgery.
The surgery is performed under general anesthesia and is laparoscopic (minimally invasive), resulting in quicker recovery times and fewer complications than an open approach. Recovery takes 4-6 weeks and patients are usually discharged after 2-3 days in hospital. Patients can start off with a soft diet and gradually start to incorporate more solid foods over the next few weeks.
A Laparoscopic Heller Myotomy is a minimally invasive surgical procedure used in the treatment of achalasia patients. It involves dissection of the muscles of the lower esophageal sphincter, thus allowing food and liquids to enter the stomach (1). The surgery is often conducted in conjunction with a Nissen Fundoplication (where part of the stomach is wrapped around the distal end of the oesophagus to prevent reflux) as gastro-oesophageal reflux disease is a relatively common complication of the procedure (2).
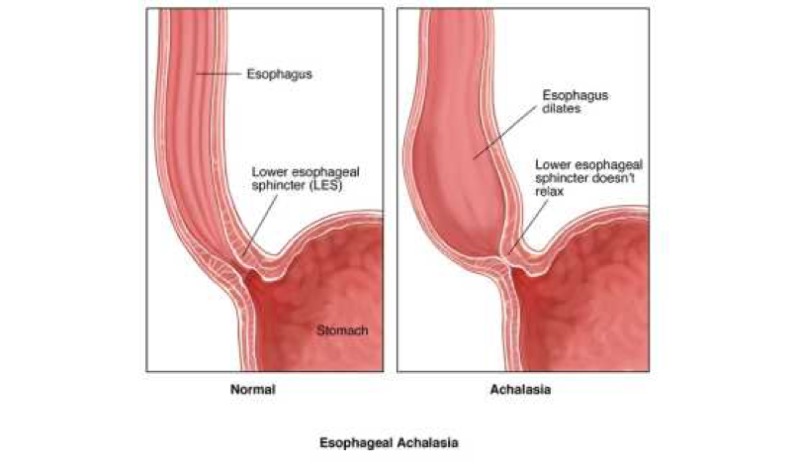
Laparoscopic Heller Mytotomy is conducted to treat achalasia, which is a functional disorder where the lower esophageal sphincter fails to relax and there is a lack of coordinated peristalsis (contractions) of the oesophagus. This causes food and liquid build up in the oesophagus and prevents food from passing into the stomach for digestion. The cause of achalasia is not fully known but its signs and symptoms are well recognised. It is one of the main causes of dysphagia (difficulty swallowing) and typically results in:
- Chest pain - This is often due to reflux and regurgitation of the food.
- Weight loss - Not all the food you eat may get digested as it is prevented from passing into the stomach.
- Dysphagia - You may feel as if food is getting stuck on its way down to the stomach (3).
Laparoscopic Heller Myotomy is thought to be one of the most definitive and long-lasting treatments for achalasia. Pneumatic balloon dilatation and botox injection alongside medical treatment using calcium channel blockers can also be used for initial therapy as they are less invasive, however the effects of these procedures are typically short lived and require repeating. Hence surgery may be required for a longer lasting solution (4).
Laparoscopic Heller Myotomy is also a minimally invasive procedure (keyhole surgery) and has been shown to result in fewer complications, lower mortality, and quicker recovery period than an open approach where a laparotomy is required to open up the abdomen. An open approach to the surgery is only performed for patients who have had many previous abdominal surgeries and hence may not tolerate a laparoscopic approach (5).
Laparoscopic Heller Myotomy is considered as the best and most employed treatment for those with symptomatic achalasia, and the other treatment options are generally used if you are not a candidate for surgery due to other factors that may affect your general health (6).
If your doctor suspects achalasia, you will have specialised tests conducted to confirm the diagnosis. These include:
- Manometry - This procedure involves passing a small tube down either your mouth or nose and measures the coordination and strength of muscle action at various points of your oesophagus and allows the surgeon to detect if there is a failure of the lower esophageal sphincter to relax.
- Barium Swallow - For this procedure you will be made to drink a special liquid and then undergo an X-Ray scan. If achalasia is present, the fluid will show as being collected in your oesophagus without moving into the stomach.
You will be required to be nil by mouth starting the night before your surgery and can only take small sips of water in the morning (7).
The surgery will be conducted under general anaesthesia and hence you will be unconscious during the procedure. For this reason, an endotracheal tube will need to be placed into your mouth and throat to help you breathe during surgery. Before the operation, you will have an appointment with the anaesthetist who can go through on the day procedures. This is also a good opportunity for you to ask any questions or address any concerns you may have.
On the day of your surgery you will be given a gown to wear alongside special stockings to prevent any blood clots forming in your legs during the surgery (Deep Vein Thrombosis). You will be taken to the operating room where an intravenous drip will be inserted into your hand/arm, and monitoring equipment such as ECG leads and blood pressure cuffs will be placed on you to measure your vital signs.
Laparoscopic Heller Myotomy is nearly always performed in conjunction with Nissen Fundoplication (wrapping the top part of the stomach around the distal end of the oesophagus) to prevent reflux that results from destruction of the lower esophageal sphincter mechanism. This occurs as food is no longer prevented from passing from your stomach into your esophagus, and hence the fundoplication is used to strengthen the distal end of the oesophagus to prevent reflux.
The steps of the procedure are as follows:
- After being anaesthetised, you will be placed on the operating table in the relevant position. There is a choice of three possible positions including:
- The supine position (lying on your back)
- Split leg position
- Lithotomy position
The split leg position (see diagram below) is commonly used, with the surgeon standing between your legs, however the supine position is also widely used. The choice of positioning ultimately depends upon surgeon preference.
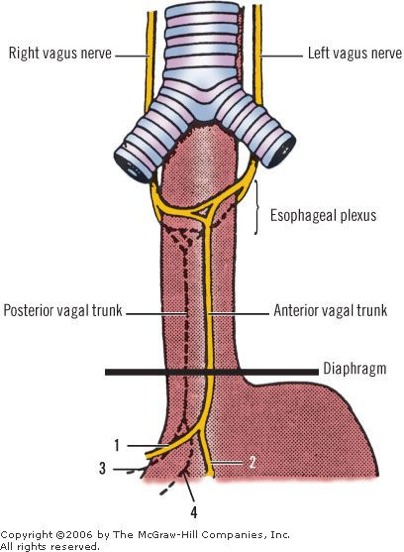
The surgeons will take care to avoid key structures when performing the surgery. There are many key structures that are closely associated with the oesophagus, including the anterior vagus nerve. Inadvertent disruption to this nerve can result in disruption to the function of multiple internal organs such as the stomach and liver. It is for this reason that gaining good exposure to the area is essential, and hence a total of five incisions are made: - The first incision allows access to the abdomen and is made in the upper left quadrant just below your lower left rib. - A further four incisions are made which will be the main ports for the operating equipment. A laparoscope will be inserted through one of these incisions. This is a thin tube with a camera on the end, connected to a TV screen on which the surgeon can use to conduct the surgery.
At this stage, gas may be pumped into your abdomen. This allows it to inflate and gives the surgeon a better view of the inside of your abdomen. 1) The first stage of the laparoscopic Heller Myotomy is to mobilise the gastric fundus, which involves gaining access to the top of your stomach which sits next to the distal end of the oesophagus. 2) The ligament that connects the stomach to the diaphragm (phreno gastric ligament) is first divided by dissecting the short gastric arteries. These run from the lower end of the spleen. The ligament that connects the stomach to the liver (gastrohepatic ligament) is then cut while taking care to avoid injury to any of the hepatic arteries which supply the liver with blood. 3) Any abdominal connective tissue covering the front of the oesophagus is dissected away alongside dissecting the right anterior phrenoesophageal ligament, while taking care to avoid the vagus nerve which is closely associated with the anterior oesophagus.
At this stage of the myotomy, the surgeon can prepare for a fundoplication to take place after the myotomy has finished by creating a posterior esophageal window. The surgeon then moves to mobilise the distal portion of the mediastinal oesophagus which lies above the diaphragm. This is done to allow for sufficient esophageal exposure on which to conduct the myotomy and prevent any tension during the fundoplication. After ensuring the anterior vagus nerve is cleared from the oesophagus, a continuous myotomy dissection is made for 6cm on the distal end of the oesophagus alongside a 3cm incision into the stomach. The incision can be started on either the stomach or oesophagus based on surgeon preference. Bleeding may occur during the myotomy incision, in which case pressure may be applied to control it. The longitudinal muscles are dissected first, followed by dissection of the circular muscle layers. Using the camera on the end of the laparoscope, inspection is performed to check for any mucosal perforations which may complicate the surgery. Fundoplication can now be performed to prevent any reflux from occurring post operation. Following fundoplication, all equipment is removed and any incisions are closed using sutures (8).

Following the laparoscopic heller myotomy, you will be taken to a recovery room as you wake up. Here, your vital signs will be monitored and when stable you will be transferred to the ward to recover. You can start drinking clear liquids on the night of the procedure, and if no complications arise you can start to eat a soft diet the next day.
You may feel nauseous after the procedure, in which case you will be prescribed antiemetics to help prevent any vomiting which may rupture the myotomy repair and fundoplication. Immediately after you wake up you may feel pain in your shoulders. This occurs due to the gas that was pumped into your abdomen during the procedure. Pain control for the shoulder pain and any incision pain is available to be taken.
You will stay in hospital for around 2 days before being discharged. This allows the doctors to monitor you and to ensure that no perforation has occurred during the surgery. If signs of perforation are present, such as chest pain, fever, and a fast heart rate, the medical team may conduct a barium swallow followed by a scan which will allow them to check for any perforation in the gastro-intestinal tract. You will be encouraged to get active and walk around either on the day of your surgery or the next day; this reduces the risk of complications such as clot formation in your legs and chest infections.
If the stitches used to close the incision are non-dissolvable, you will be required to visit the GP surgery to have them removed, usually 7-10 days after the operation.
You will be required to eat a soft diet for approximately 2 weeks following the surgery to allow the repair to heal. This can include foods such as:
- Soup
- Smooth yoghurt
- Ice cream
- Porridge
- Scrambled eggs
- Custard
You may have difficulty swallowing for the first 5-7 days however this is expected to get better over time. Before discharge, the medical team will speak to you about tips for eating including taking small mouthfuls and chewing for a long time before swallowing.
As you start to feel more comfortable eating a soft diet, you can gradually begin to eat more solid foods which may take a few weeks. To ensure that swallowing is as smooth as possible, ensure you drink plenty of fluids and avoid fizzy drinks as this may make you feel bloated.
Its a good idea to have someone stay with you for one night once you are discharged if you live alone.
You may feel pain for the first few days after discharge, hence you will be advised to take regular painkillers. Breathing may be difficult or painful after having a major surgery such as a myotomy; and hence while you are in hospital, the nurses and physiotherapists will work with you to ensure your lungs recover and to prevent collapsing of the lung due to insufficient breathing (atelectasis). Painkillers can also help to relieve some of the pain and help you breathe deeper (9).
This will all be explained by the professional during your stay.
It is common to need a couple of weeks or recovery at home after this procedure.
Comments