Hip Replacement/ Hip Arthroplasty

Introduction
What is it?
Hip replacement, or Total Hip Arthroplasty is a very successful orthopaedic operation. The British surgeon Sir John Charnley developed the technique and the first implants used. A hip replacement is very effective in relieving pain from the hip and can improve function and impact positively on quality of life.
The hip joint is a ball and socket type of joint. The Total Hip Arthroplasty operation changes both the ball and the socket to artificial replacements (prosthetics/ implants).
There are a few technical consideration which make the operation performed different:
1. Material used in Artificial Joint
Cups and Stems: The cup is the replacement socket part of the new hip joint. The stem is the new ball which is attached to the thigh bone and fits into the new socket. These are usually make of titanium.
New joint surfaces - bearing surfaces: Most common these days is a Polyethelene liner - this fits inside the cup. The head surface is commonly cobalt-chrome. Ceramic and metal have also been used. The various materials have pros and cons related to their individual properties.
Ultra high molecular weight Polyethelene is a good articular surface but tends to have a high wear rate and the debris produced causes loosening of the join (aseptic loosening). Sterilisation of the material in an oxygen free environment promotes cross linking of the Polyethelene resulting in much less wear.
Cobalt-chrome is a 'supermetal' alloy. This is often used as a femoral (thigh bone) ball surface together with a Polyethelene liner to the socket.
Metal on metal implants have been used. The debris is much smaller with metal resulting in less chance of loosening but stimulating cancer is possible complication.
Ceramic material for the joint surface provides excellent wear rate but is brittle and can fracture.
The size of the ball join head is also important. A larger head provides more stability to the joint, but also results in more wear. Currently a 28 mm ball size is common.
2. Technique of fixation - cemented or un-cemented
Cemented: The cement used is called Methylmethacrylate. It is most often used in older patients. It advantage is that is creates an immediate strong and stable fixation. Cement tends to work better when compressed than when put in tension. Hence the femoral (thigh bone) component tends to do better than the acetabular cup part.
Un-cemented/ Biological: This is more popular in younger patients. Your own town grows onto to into the implant. When first implanted there needs to be another way of creating immediate fixation until the bone grows in. This can be done by using an implant a couple of millimetres bigger than the size of the bone. Alternatively, the exact size can be used and screws are used to hold it in place which the bone grows in.
3. Operative approach to the hip joint - which route to take to get to the hip joint.
The 'approach' refers to where the cut is made in the skin and which muscles and other structures are moved and cut to get to the hip joint to do the replacement. There are various pros and cons relating to the types of approach.
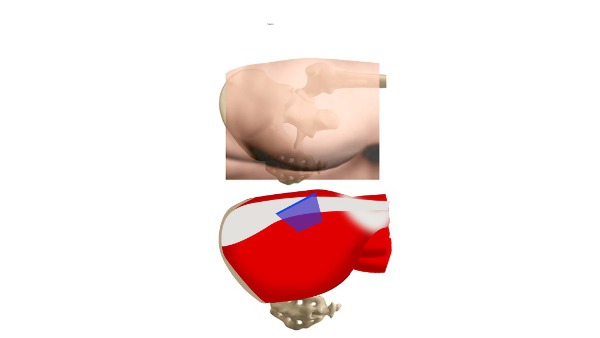
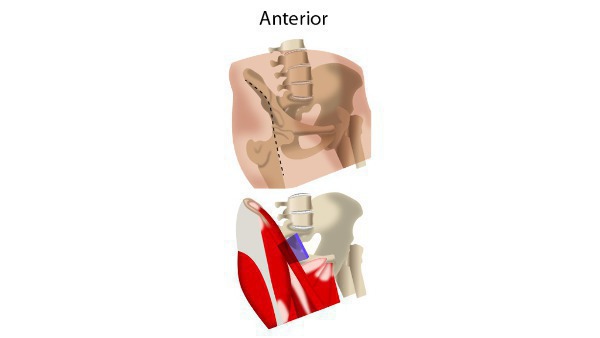
The anterior approach is when the surgeon makes a cut at the upper part of the pelvis as the patient lies on their back on the operating table. The posterior approach is when the surgeon makes a cut behind part of the upper thighbone as the patient is lying on their side (1).
The anterior approach may have earlier recovery time; a shorter incision length and reduced blood volume loss than the posterior approach (2)
Posterior approach (Moore/ Southern) to the hip joint.
This approach involves splitting the gluteus maximus muscle in the buttock and cutting a number of muscles which externally rotate the thigh bone. These are repaired at the end of the operation to prevent the hip dislocating backwards. There is a potential advantage of protection of the sciatic nerve which runs close to the hip joint at the back.
Lateral approach (Hardinge) to the hip joint.
The gluteus medius muscle is split and pushed apart to reveal the outer surface of the hip joint. This approach may result in less risk of dislocation after surgery.
Anterero-lateral approach (Watson-Jones) to the hip joint.
Here, a space between the tensor facia lata and the gluteus medius is created by pushing those two muscles apart. The abductor muscles must be detached from the femur to get to the hip joint. There is a potential risk to the femoral nerve using this approach as it needs to be pushed out of the way of the surgery.
Why is it done?
Conditions that damage the hip joint to the point where you may require hip replacement surgery include:
Osteoarthritis(OA) - Wear and tear disease of the smooth cartilage that covers the bone end at a joint helping it to move smoothly.
Rheumatoid arthritis(RA) - Autoimmune disease that causes inflation and erodes the cartilage and underlying bones resulting in deformed joints.
Osteonecrosis - Inadequate blood supply to the hip joint resulting in bone collapse and deformation.
These conditions are initially treated with medications and physiotherapy, but ultimately requires arthoplasty when hip pain: Persists, despite pain medication Worsens with walking, even with a cane or walker Interferes with your sleep Affects your ability to go up or down stairs Makes it difficult to rise from a seated position.
Will I need to do any preparation?
Your symptoms are most important in terms of decision making regarding having a hip replacement. Together with the results of clinical examination, blood test and an X-ray and possibly an MRI, an overall picture is developed regarding need for surgery.
Your bodies ability to deal with the stress of surgery will also need to be assessed. This is often done in pre-admission clinics where relevant tests and your fitness are considered.
Technique
Anaesthesia
The operation is commonly performed under general anaesthetic which the patient will be asleep during the operation. The operation can be performed using an epidural or spinal anaesthetic which only acts on the lower body.
What does it involve?
The operation can be divided into two parts, one to deal with he acetabulum and another to deal with the Femur (thigh bone).
Anterior approach
The patient is positioned so they are lying on their back so that the surgeon has access to the front of the leg. A cut is made at the top of the leg underneath one of the bony prominences on the front of the pelvis. One of the muscles (tensor fascia lata) in the leg is cut to provide access to the joint. The surrounding ligaments and fatty tissue are removed to expose the bone.
Posterior approach
The patient is positioned so they are lying on their side so that the surgeon has access to the back of the leg. A cut is made at the top of the leg.
One of the muscles (gluteus maximus) in the leg is cut to provide access to the joint. The surrounding ligaments and fatty tissue are removed to expose the bone. The socket of the joint (acetabulum) is replaced with an artificial cup.
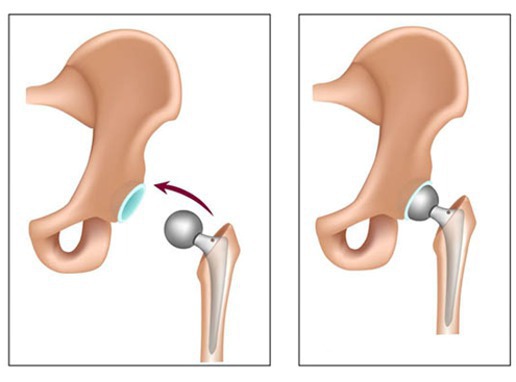
Femoral part
The head of the femur (thighbone) is removed and an artificial head is inserted.

Acetabular part
The socket of the joint (acetabulum) is replaced with an artificial cup.

'Reducing' the joint back in place
The wound is closed with stitches and dressed.
How long does it take?
The operation usually takes 1-2 hours to complete.
Post procedure course (follow-up)
Surgery is followed by early mobilization, this is important to minimise complications.
Elastic compression stockings or inflatable air sleeves are worn on the legs and blood thinning medication is taken to reduce the risk of blood clotting in the legs. a major risk after Hip Arthoplasty.
How long will I stay in hospital?
People often stay in hospital for up to 3-5 days. The team will assess how the new hip is functioning and advise a personalised rehabilitation plan for the following months to help recovery. This will involve a physiotherapist and an occupational therapist.
What care will I need at home?
Some may require inpatient rehabilitation in a dedicated rehabilitation unit or nursing home. Mobilisation and physical therapy begin as soon as possible to speed up recovery and reduce risk of deep vein thrombosis (DVT).
Enhanced recovery protocols are commonly used with targets to achieve every day. Rehabilitation exercise may involve 20 to 30 minutes two or three times daily during initially. You are allowed to weight bear as soon as tolerated is allowed.
Will I need someone to stay with me?
Depending on your level of function when you go home, you may need someone to help you with your daily activities. Your needs are professionally assessed by a physiotherapist and occupational therapist before discharge from hospital.
Will I need any special equipment when I go home?
Assist devices and walking aids (Zimmer, rolator frames or crutches) are used to help with balance and stability. Walking aids are weaned off as strength, balance, and comfort improve.
What follow up care is needed?
6 to 12 weeks after surgery, you'll have a follow-up appointment with your surgeon to make sure your hip is healing properly. If recovery is progressing well, most people resume their normal activities by this time — even if in a limited fashion. Further recovery with improving strength will often occur for six to 12 months.
When can I start my normal activities again (e.g. driving, sports or work?)
The doctor or physiotherapist will be able to advise on when it is safe to return to normal activities which can differ from patient to patient. A rough guide is 6 weeks before returning to light activities and driving. Improvement may continue for up to a year.
Alternative treatment options
Conservative Treatment:
Patients who have severe arthritis of the hip, but function adequately, can choose to live with their condition Among these are physical therapy, walking aids, anti-inflammatory medications, cortisone injections, and joint supplements.11 Hip Resurfacing Hip resurfacing surgery is an alternative to standard hip replacements for patients with severe arthritis. In a hip resurfacing surgery, the implant is smaller, and less normal bone is removed. Hip resurfacing is gaining interest, especially in younger patients.11 Partial Hip Replacement (Hemiarthroplasty) In this procedure only ball of ball and socket joint of hip is removed good alternative in case of trauma specially in young patient but poor outcomes in hip arthritis as this procedure donot addresses the socket part of the joint.11 Hip Fusion (Arthrodesis) Hip fusion is rarely done because of the growing success of hip arthoplasty involving fusion of hip bone and femur preventing any movement at hip joint at the cost of less post operative movement rehabilitation procedures.11 Resection Arthroplasty (Gridlestone Procedure): A resection arthroplasty is a procedure where the bone around the hip joint is removed and the joint space is allowed to fill with scar tissue. This procedure is usually done in patients with a severe infection that cannot be controlled, or in patients whose physical condition is such that they have little chance of normal walking. Patients who undergo a Girdlestone resection arthroplasty will likely need some device (crutches or walker) for walking. Hip Osteotomy Hip osteotomy is a procedure that is done to realign the bones of the hip joint. The osteotomy can be performed on the thigh bone (femur), the pelvis, or both. Osteotomies are usually performed on patients with an underlying problem that has led to early arthritis of the hip joint. For example, developmental conditions such as hip dysplasia can lead to early hip arthritis. Hip dysplasia occurs in infants and leads to misaligned bones around the hip. The osteotomy helps to realign the bones and relieve the symptoms of early arthritis. These procedures must be done in carefully selected patients.




Comments