ERCP (Endoscopic retrograde cholangiopancreatography)

Introduction
What is it?
Endoscopic retrograde cholangiopancreatography or ‘ERCP’ is a procedure that is used to look at the drainage channels (bile ducts) arising from your liver and pancreas. It is performed by a specially trained doctor called an endoscopist to diagnose and treat conditions of the biliary tract. Treatment of conditions using ERCP depends on the problem. For example, gallstones can be removed using a small cut to the duct to allow passage of stones, or stents can be placed in bile ducts where there is a narrowing.
What is the biliary tract?
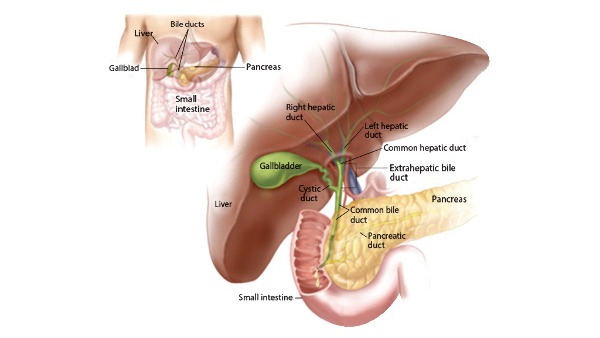
The biliary tract contains the organs and channels that produce and store bile. The main role of the biliary tract is to allow the flow of bile from the liver into the first part of the small bowel (the duodenum) where it helps in the digestion of food. Some bile is stored in the gallbladder for later use. The biliary tract starts with many small branches in the liver which join together to form bigger branches eventually all leading to a channel called the common bile duct. For this reason, it is sometimes known as the ‘biliary tree’. The common bile duct allows bile to flow into the small bowel through a small hole called the papilla. This is the point where the pancreatic duct also allows pancreatic juice to enter the small bowel.
What is Bile?
The liver produces around 600ml of bile a day. Bile is a yellowish green liquid which contains substances needed for digestion of fats in particular. Bile flows from the liver into the digestive tract through a system of channels called bile ducts. Bile is responsible for the brown colouration of our faeces. In some conditions if there is a blockage of bile reaching the intestine, faeces can become pale/whitish as not enough bile is reaching the gut and instead overflows into the blood steam resulting in yellowing of the skin (jaundice)
Why is it done?
An ERCP is a procedure that can be used to diagnose and treat certain conditions of the biliary system. Conditions of the biliary system can result in a number of symptoms including jaundice (yellowing of the skin), weight loss, abnormal bowels, abdominal pains, and infections.
An ERCP in most cases is performed when evidence of abnormal blood tests or scans of the abdomen (ultrasound or CT) point to cause. The most common reason for an ERCP is for the treatment of gallstones causing a blockage of the bile ducts. Often this is the situation when pre-operative tests are being done for a patient about to have a laparoscopic cholecystectomy.
Other indications for ERCP (from the British Society of Gastroenterology guidelines): 1. Bile duct stones 2. Jaundice due to a stricture (narrowing) of the lower bile ducts in patients not suitable for an operation 3. Hilar biliary stricture (narrowing of the bile ducts entering the liver) 4. Bile leak or jaundice following a cholecystectomy (gall bladder surgery) 5. Pancreatic duct stricture (narrowing) causing symptoms 6. For biopsies 7. Emergency treatment of cholangitis (infection of the bile ducts causing sepsis
Will I need to do any preparation?
Preassessment Clinic You may be seen by a nurse or doctor in a pre assessment clinic a few weeks prior to the ERCP. Your full medical history will be obtained and your suitability for the procedure will be determined following this. Any medications that need to be stopped or changed will also be addressed. Patients with the following conditions should ensure they let the doctor know prior to the procedure • Diabetes • Haemophilia or other blood disorders • Pacemaker or other implant • Blood thinning medications • Heart or lung diseases Pregnancy
Although ERCP can be performed safely during pregnancy, this is usually reserved for urgent indications. Most non urgent cases are postponed until after child birth. Medications Some medications may need to be stopped prior to having an ERCP. Blood thinning medications (e.g Aspirin, Clopidogrel, Warfarin, Enoxaparin, Rivaroxiban, Apixiban etc..) may need to be held to reduce the risk of bleeding during and after the procedure. You should discuss this with the doctor well in advance of the ERCP to allow time to plan. Sometimes the doctor will need to take advice from other specialists when holding certain mediations. Certain diabetic medications may also need to be stopped or adjusted on the morning of the procedure as you will not be eating for 6-8 hours. On the day Nil by mouth You will be asked to remain ‘Nil by mouth’ for six to eight hours before the procedure. This means you should not eat or drink during this time. This is to allow the doctor to visualise the structures clearly (without food being present in the gut) and also to reduce the risk of vomiting.
Technique
Anaesthesia
You will be given a local anaesthetic throat spray to help numb your throat. This also decreases the gag reflex when the endoscope is passed into your food pipe. In most cases conscious sedation is used, however in some units and in complex cases, a general anaesthetic is used.
Sedation
Most ERCPs are performed under ‘sedation’. An intravenous cannula (small tube to allow administration of medications) will be inserted into one of the veins in your hand or arm. Most endoscopy units use a sedative medication to cause relaxation in addition to medication to relieve pain. This is called ‘conscious sedation’ as you will not be asleep.
General Anaesthetic
Some units and in ore complex cases you may require a general anaesthetic – where an anaesthetist will use medication to put you asleep.
What does it involve?
Before the Procedure: 1. Arrival to the Endoscopy Unit. If you are an inpatient you will usually be escorted by a nurse to the endoscopy unit. This is a designated part of the hospital containing rooms that are used for endoscopic procedures. If you are an out-patient you will be asked to report to the unit at a specific time. You may have to wait in a waiting area until you are seen by an endoscopy nurse who will go through a few identity checks and medical history with you. You will be given a hospital gown to change into.
2. Consent Form Before the ERCP you will be seen by the endoscopist who will also go through your medical history, blood results and any recent scans that you may have had. The endoscopist will explain the procedure in full, discussing the benefits and risks of ERCP. You will be asked to sign a consent form.
3. Endoscopy room. ERCP is performed in an endoscopy room containing x ray equipment. This is because as describe earlier, x rays are used to examine the bile ducts following injection of a special dye into them. The room will also contain monitors which are connected to the camera on the endoscope which is essential for the doctor to visualise the digestive tract.
4. Monitoring You will be attached to some monitors before the procedure, to measure your blood pressure, heart rate, heart rhythm and oxygen levels.
The Duodenoscope
The ERCP endoscope is called a duodenoscope. It is an advanced flexible tube which is approximately the same width of an index finger. It contains a small camera and a light allowing the doctor to see the inside of the digestive tract on a monitor. The endoscope contains channels that allow insertion of a variety of instruments – to take biopsies, withdraw fluid, introduce air, introduce cutting devices and stents.
The procedure:
1. You will be asked to lie on a special bed on your left side or belly.

2. A mouth guard is inserted between the teeth – this prevents damage to the teeth and the endoscope.

3. The endoscope will be inserted into the mouth and you will then be asked to swallow it. Most people do not have difficulty with this due to the sedating mediations given. One the endoscope has been inserted, air is gently introduced to inflate the oesophagus, stomach and intestine so that it can be passed through with ease. 4. Once the papilla has been reached (the opening of the bile ducts into the intestine) a cannula (small plastic tube) is inserted through this opening and a special dye is injected.
5. X rays are taken after the dye has been injected which allow examination of the bile ducts and pancreatic duct.

How long does it take?
6. If any intervention or treatment is required, sometimes a sphinterotomy is required. A spincterotomy involves cutting of the muscle at the mouth of the papilla. This allows for the hole to be widened up an allow instruments to be passed into the ducts.
How long does it take?
The procedure takes between 30 mins to over 3 hours, depending on the procedures or complexity of the case. Longer treatment times are usually if procedures like stone extraction or stent placement are done.
Post procedure course (follow-up)
When can I eat and Drink?
Usually you may eat and drink once you are fully awake, however in some cases you may be required to continue to fast for a further period of time. The doctor performing the procedure will write a set of notes detailing your post procedure care which would have been given to the nurses and doctors looking after you.
Do I need someone to take me home?
If you are going home you will require someone to escort you as the sedation takes time to wear off you will not be able to drive.
Should I take my usual medications after the procedure?
You should continue to take your usual medications unless instructed by your doctor. If any medications have been stopped – the doctor will inform you when it is safe to restart these.
Can I drink Alcohol?
You should not drink alcohol for at least 24 hours after the procedure as the sedation can take time to wear off. Discuss this with your doctor.
How long will I stay in hospital?
Following the procedure you will be monitored in the recovery area by nurse who will assess your blood pressure, oxygen levels, temperature and heart rate regularly. You will usually remain in the unit until you are fully awake which takes about one hour. Following this you will be observed for a further 6 hours following the procedure
What care will I need at home?
No particular care required.
Will I need someone to stay with me?
It is advisable to have somebody with you for at least 24 hours until the sedation has worn off.
Will I need any special equipment when I go home?
No routine special equipment us needed unless otherwise you are told otherwise.
What follow up care is needed?
When can I start my normal activities again (e.g. driving, sports or work?)
Sedation can sometimes last longer than you think. During the first 24 hours after the procedure you should not drive, ride a bike, operate machinery or do anything that requires a skill. You should also not drink alcohol, take sleeping tablets or make important decisions.



Comments